

{kind=link}
Introduction
Health methods are at all times confronted with key challenges in relation to main healthcare. These embrace creating and retaining workforce, data administration, financing the well being sector and truthful provision [1], distribution of infrastructure and useful resource allocation administration [2, 3], affordability, availability and accessibility of well being providers [4–6], and matching providers to the wants of the general public [7, 8]. Based on researches entry to well being providers is a multi factorial concern and depending on many differ determinate elements together with: presence of services, personnel inhabitants density, socio-economic standing, funds required, transport, willingness of well being providers to simply accept cultural minorities, bodily accessibility for folks with disabilities, gender issues, and cultural attitudes and beliefs about well being providers and their usefulness. Besides, greater entry and use of well being providers is extra wanted for some in danger teams equivalent to: moms, infants, older folks or others within the inhabitants whose well being is comparatively extra at risk- for instance these with continual well being circumstances [9–14]. In a scenario the place the supply of providers is historically measured by indexes such because the variety of physicians and hospital beds per unit of inhabitants [15], the truthful distribution of well being providers has at all times been one of many main issues of well being methods worldwide [8, 16]. Not to say, regardless of the rising charge of financial progress and dramatic advances within the well being sector within the final century, there are nonetheless large inequalities on this respect [17–19], and this has even been one of many essential challenges in developed nations [20], particularly in Iran [21].
Access to healthcare providers is a prerequisite for creating fairness within the well being of societies, and the fitting to healthcare will create equal alternatives in societies [22]. Furthermore, laying the groundwork for the equitable enjoyment of health-related interventions is essentially the most vital work that the well being system can take to attain social justice by way of well being. It needs to be famous that wellbeing shouldn’t be one thing that may be distributed instantly amongst folks. From the angle of well being, ‘social justice’ denotes justice within the distribution of well being in society, which is why the well being policymakers and stake holders primarily based their methods on the truthful distribution of the determinants of well being [23, 24]. Since unbalanced distribution of providers results in the inefficiency and inappropriate service provision [17, 24] (e.g., imbalances in well being workforce by way of amount, high quality, and distribution), can have penalties for well being [25]. In 2008, the world well being group (WHO) introduced that each one folks ought to have entry to healthcare in accordance with their wants, no matter their fee energy [26]. The lack of correct entry to medical care in societies has resulted in adverse penalties, equivalent to social inequity, elevated illness, rising mortality from diseases, accidents and unbalanced distribution of providers [17, 24, 27].
Research signifies that inappropriate focus of services and medical care is seen as a serious drawback in lots of nations [8, 24, 28–32]. This drawback has additionally been noticed in Iran [25]. Similarly, in Iran, Shahabi et al. [33] reported that the privileged provinces have been thrice higher than the underprivileged ones by way of the ratio of physicians, hospital beds, laboratories and radiology providers to the inhabitants. In one other comparable research carried out by Mehrjardi et al. [34], the standing of growth and rating of Iranian provinces have been addressed by way of entry to the indexes of the well being sector. The outcomes of their analysis revealed that amongst 30 provinces of Iran, 12 have been developed, 9 have been semi-developed, and 9 have been underdeveloped, of their categorization, Kermanshah Province was among the many semi-developed provinces [34]. Studies carried out in Kermanshah the excessive vital charges for HIV/AIDS [35], most cancers [36], cardiovascular ailments [37], accidents [38], excessive complete fertility charges [39], and insufficient entry to well being facilities [11]. Such evidences revealed the necessity for assessing healthcare assets and surviving the entry to those cares.
Since rising the extent of well being and quick access to medical care are among the many most distinguished wants in growth plans and contemplating the truth that the Kermanshah Province is without doubt one of the disadvantaged provinces of Iran and given the prevalence of the above talked about challenges in Kermanshah, this paper aimed to research the inequality in entry to medical care within the townships primarily based in Kermanshah, Iran in response to inhabitants density.
Materials and strategies
Study design
In this research, the coefficient of variation of the ratio of entry indexes to the medical care to a inhabitants of 10,000 residing in townships was employed as an index for exhibiting the dearth of uniformity [40]. More to the purpose, the upper this index, the higher the dispersion of the above-mentioned variable can be. This index is calculated as follows [41]:
CV = Coefficient of variation
Standard deviation = σ
Mean = μ
The diploma of growth of the townships was calculated by way of entry to medical care utilizing the hierarchical cluster evaluation (HCA) via the Ward Algorithm [42], and the mixed mannequin of human growth index (HDI) [43]. In this regard, the townships have been categorized in response to these indices into 3 teams as disadvantaged, creating and privileged teams, respectively.
The general construction of the HDI Model is proven as follows in Formulae 2.
Maximum worthXi-Actual worthXiMaximum worthXi- Minimum worthXi =Xi (2)
WhereXirepresents the indexes used within the HDI mannequin [43].
The second stepwise the definition of the imply index for every of the townships for reaching this purpose Formulae 3 was utilized.
In this formulae Xj represents the common index for every township, and Xi represents the indexes used within the HDI Model.
The third step of this technique was to calculate the human growth which its worth is between zero and one (the nearer the obtained worth to 1, the extra developed it is going to be) [43]. This was assessed by Formulae 4.
The checks have been employed to establish the deployment sample of the standing of accessing to medical care indexes throughout the Kermanshah-based townships have been together with: Mean Center and Standard Distance.
(A) Mean Center: It is the imply of geographical latitude and longitude coordinates of all options inside the scope of the research, and its calculation is suitable for each monitoring the modifications within the spatial distribution of terrains and their comparisons. It is calculated as follows [11]:
X̄=∑i=1nxin,Ȳ=∑nnyin (5)
Where Xi and yi are the coordinates for characteristic i, and n is the same as the entire variety of options.
(B) Standard Distance (SD): It is a technique for analyzing the extent of focus or dispersion of geographic options across the imply heart and is calculated as follows [11]:
SD=∑i=1n(xi−X−)2n+∑i=1n(yi−Y−)2n (6)
Where xi and yi are the coordinates of characteristic i, {X-,Y-}represents the imply heart for the options, and n is the same as the entire variety of options.
Not to say, all spatial processing was carried out utilizing the Arc GIS 9.3 Software.
Results
The findings confirmed that there have been 16.55 nursing workers, 6.73 paramedics, 11.97 well being care personnel, 2.48 common practitioners, 2.51 specialists, 1.29 dentists and 0.16 pharmacists per 10,000 folks in Kermanshah Province in 2011. There have been additionally (0.11) hospitals, (13.24) lively hospital beds, (0.20) clinics, (0.02) specialised clinics, (0.15) common clinics, (0.30) radiology wards, (0.31) rehabilitation facilities and (0.66) labs per 10,000 folks (Table 1).
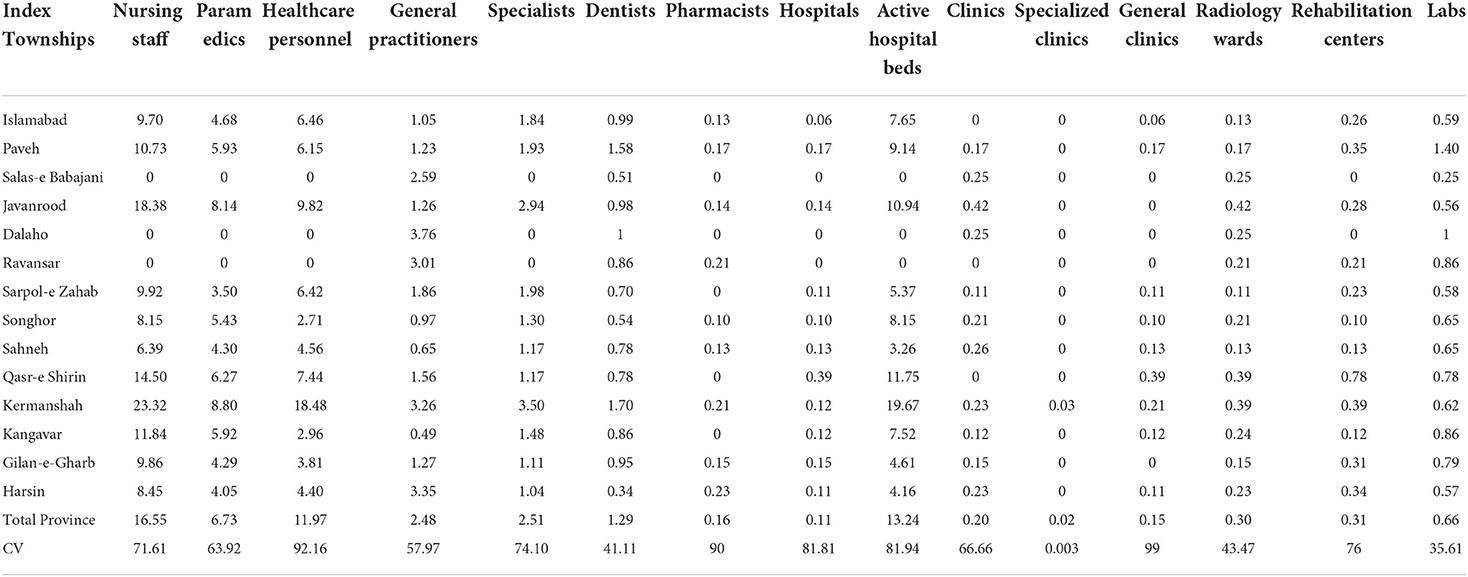
Table 1. The distribution of well being professionals and remedy services per 10,000 folks within the townships of Kermanshah Province.
In phrases of the ratio of nursing workforce to a inhabitants of 10,000 in townships, it was discovered that the most important variety of nursing workers belonged to Kermanshah Township (23.22) and the smallest numbers belonged to the townships of Salas-e Babajani, Dalahu and Ravansar. The largest variety of paramedics per 10,000 folks belonged to Kermanshah (8/80), whereas Salas-e Babajani, Dalaho and Ravansar had the fewest paramedics. Furthermore, Kermanshah held the very best variety of administrative personnel in healthcare per 10,000 folks (18.48), versus the bottom numbers within the townships of Salas-e Babajani, Dalaho and Ravansar (Table 1).
In phrases of the ratio of common practitioners in numerous townships, Dalaho and Kangavar had the very best and lowsest ratios (3.76 and 0.49, respectively). Moreover, the most important variety of specialists have been in Kermanshah (3.50), whereas Dalaho, Salas-e Babajani and Ravansar had the fewest specialists (Table 1).
The ratio of dentists to a inhabitants of 10,000 in every townshipwas one other index that reveals the distribution of dental workforce throughout townships. More to the purpose, Kermanshah and Harsin had the very best and lowest numbers of dentists (1.7 and 0.34, respectively) (Table 1).
The highest variety of pharmacists per 10,000 folks was in Harsin (0.23), versus the bottom numbers within the townships of Salas-e Babajani, Dalaho, SarpulZahab, Qasr-e Shirin and Kangavar (Table 1).
Paveh had the very best ratio of hospitals to 10 thousand folks (0.39), whereas Salas-e Babajani, Dalaho and Ravansar had the bottom ratios. However, by way of lively hospital beds, Kermanshah had the very best degree (19.67), versus Salas-e Babajani, Dalaho and Ravansar the place there have been no lively hospital beds (Table 1).
The ratio of specialised clinics to 10,000 folks measured 0.03 within the township of Kermanshah, whereas different townships lacked the required providers. However, by way of public hospitals, Qasr-e-Shirin had the very best ratio, versus the bottom ratios in Salas-e Babajani, Javanrood, Dalaho, Ravansar, and Gilan-e-Gharb (Table 1).
In addition, by way of the ratio of radiology facilities to a inhabitants of 10,000, Javanrood (0.42) and in Sarpol-e Zahab (0.11) had the very best and lowest ratios, respectively (Table 1).
In phrases of the ratio of rehabilitation facilities to a inhabitants of 10,000, Qasr-e-Shirin had the very best ratio (0.78), versus the bottom ratios in Salas-e Babajani and Dalaho Townships (Table 1).
In addition, by way of the ratio of laboratories to a inhabitants of 10,000, Paveh and Salas-e Babajani had the very best and lowest ratios (1.40 and 0.25, respectively) (Table 1).
Furthermore, the coefficient of variation (CV) revealed that the indices beneath research have been unequally distributed throughout the townships of Kermanshah (Table 1).
Hierarchical cluster evaluation with ward algorithm
According to the outcomes of cluster evaluation, the Kermanshah townships have been divided into three classes (disadvantaged, creating and privileged) by way of entry to well being providers. The disadvantaged townships included Ravansar, Dalaho and Salas-eBabajani, and the creating townships included Gilan-e-Gharb, Harsin, Sarpol-e Zahab, Sahneh, Islamabad, Paveh, Songhor, and Kangavar. While Kermanshah, Qasr-e Shirin and Javanrood have been among the many privileged areas (Figure 1).
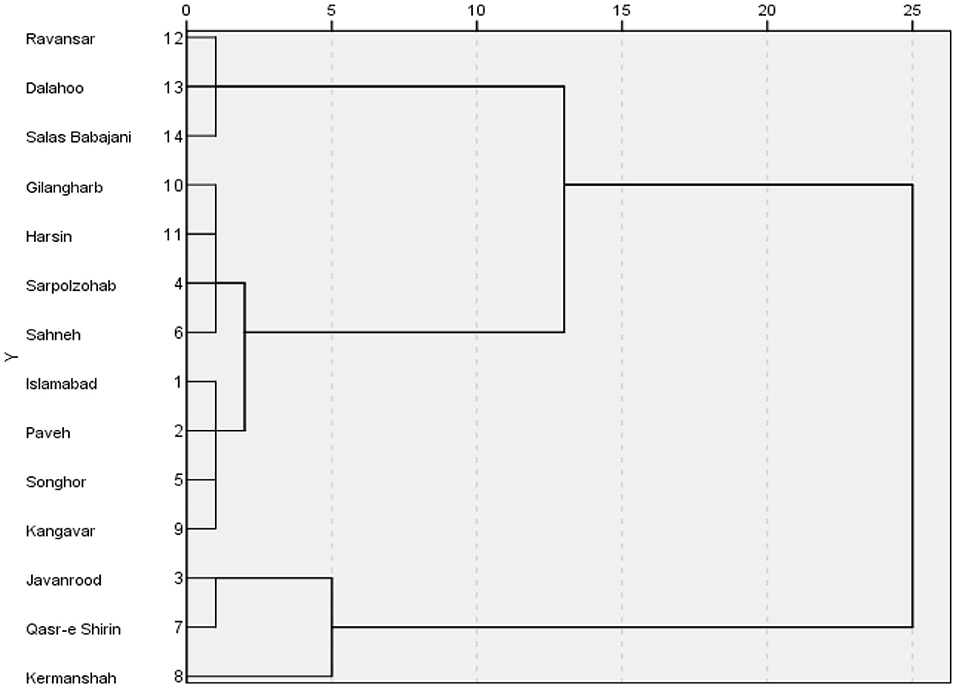
Figure 1. Cluster diagram of the indexes of entry to medical care on the townships.
Based on the mixed mannequin of HDI, the findings of the current research indicated that Ravansar, Dalaho and Salas-eBabajani have been essentially the most disadvantaged townships by way of entry to medical care (Table 2; Figure 2).
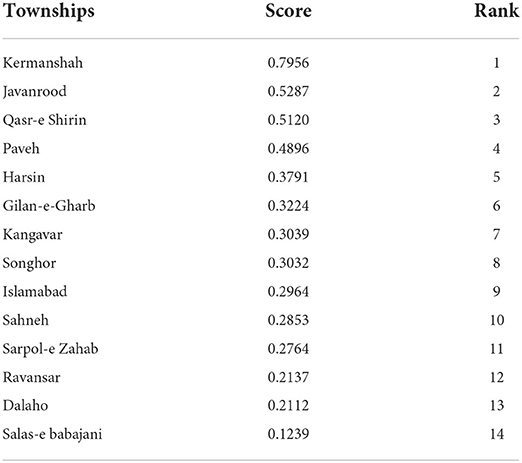
Table 2. Status of townships by way of entry to medical providers primarily based on the mixed mannequin of HDI.
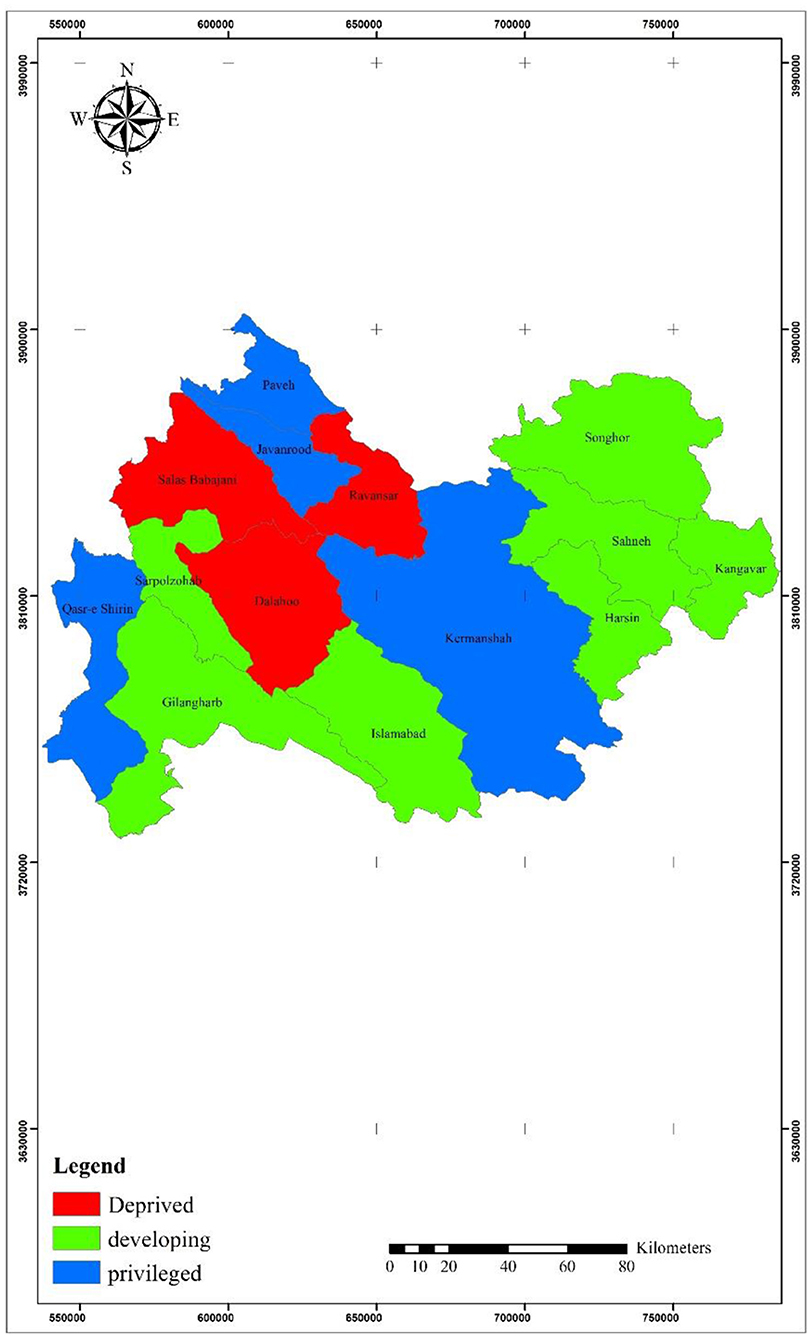
Figure 2. The standing of townships by way of entry to medical care primarily based on the mixed mannequin of HDI.
Mean heart and commonplace distance
The outcomes of measures of central tendency confirmed that the middle of the institution of well being indexes was positioned within the Kermanshah Township. The commonplace distance of the distribution sample of well being providers confirmed a excessive focus within the central areas. The elongation of the usual distance of well being providers was indicative of the truth that their accumulation was in sure locations of the province.
The outcomes of evaluating the imply facilities of inhabitants and well being services indicated that the facilities of each knowledge classes have been positioned in Kermanshah. However, the outcomes of observing the usual distance (inhabitants and well being services) confirmed that the usual distance of well being facilities was bigger. In different phrases, geographically, the well being services witnessed extra dispersion within the northwestern areas than the focus of inhabitants within the central and southeastern areas of the province (Figure 3).
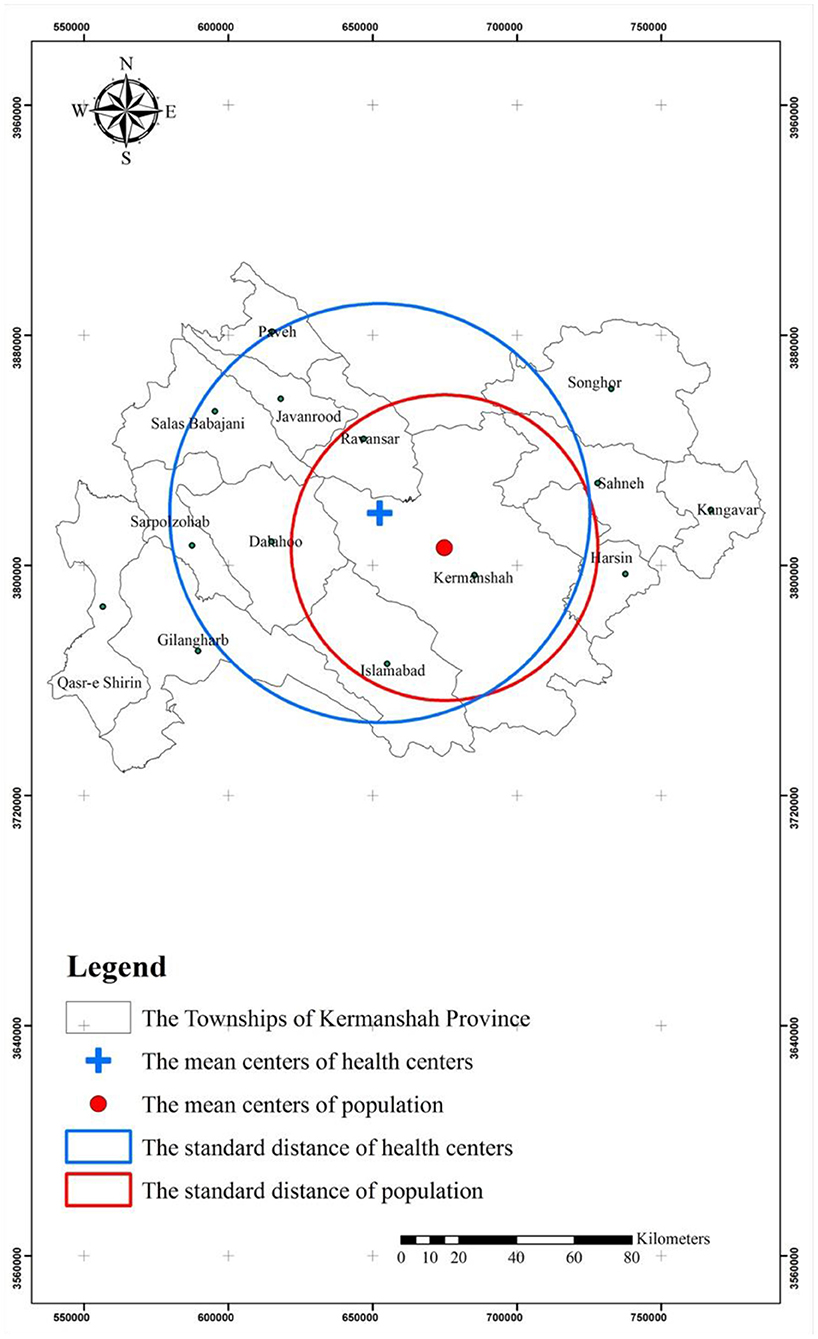
Figure 3. Spatial and commonplace distance of well being providers and inhabitants within the townships.
Discussion
Access to medical care is without doubt one of the main points affecting the human well being from totally different features. One strategy to obtain this objective in societies is the equal entry to the services of the well being sector. Therefore, the current research aimed to research inequality in entry to medical care within the townships primarily based in Kermanshah, Iran.
The outcomes of learning the established order of the distribution of well being assets in Kermanshah confirmed that there was heterogeneity on this regard, which was according to the outcomes of research stating that there have been giant gaps between totally different areas in Iran by way of this issue [9, 11, 33, 40, 44, 45]. In a research carried out by Reshadat et al. [9], it was concluded that the elements equivalent to lack of planning, fallacious policymaking by way of the distribution of well being providers, unfair distribution of economic assets and structural issues accounted for this case. In addition, the results of the 8-year conflict between Iran and Iraq, financial sanctions, political-economic weaknesses, extreme inhabitants progress, and extreme migration of villagers to cities may account for this case in Iran [46]. Besides, the well being standing of individuals in numerous well being points, together with ailments and different instances in Kermanshah can be negated by the dearth of correct entry to healthcare provides [36, 47].
In phrases of the ratio of specialists to a inhabitants of 10,000 folks, the outcomes of the current research have been indicative of an unequal distribution of services throughout the townships of Kermanshah Province. Moreover, the townships of Salas-e Babajani, Dalahu and Ravansar had the bottom ratios, versus Kermanshah with the very best ratio. This discovering was much like these carried out in different research in Iran [9, 33]. Not to say, plainly the Ministry of Health has carried out poorly by way of the distribution of specialists amongst areas, thereby resulting in a scarcity of specialised and skilled physicians all through many areas of the nation. Since in response to the World Health Organization, the ratio of physicians (common and specialist) to 10,000 folks on this planet is 15.55, whereas this index has been 4.30 and 26.80 in creating and developed nations, respectively [48]. This index measured 11.9 and a pair of.49 in Kermanshah Province and Iran, respectively (see Table 1) [49]. In addition, the outcomes of the current research have been indicative of the truthful distribution of common practitioners. In this regard, in response to the findings of research carried out in Iran, the geographical, demographic and financial, social and political elements equivalent to financial progress, tradition and beliefs and elements related to particular person and motivational traits of physicians, equivalent to age, gender, and fee system, have been discovered efficient on this regard [50].
In our research, the ratio of common practitionersto 10,000 folks was 2.48. However, a charge of 10.2 was reported for Iran by Haghdoost et al. [51]. The highest ratios of common practitioners to 10,000 folks have been in Tehran (18.7), Yazd (13.9) and Isfahan (12.20), respectively. While, the bottom ratios have been noticed in North Khorasan (3.4%), Sistan and Baluchestan (3.7) and South Khorasan (3.8), respectively [51].
The outcomes of the research confirmed that there was an inadequacy of medical personnel within the Kermanshah Province. Hence, it’s vital for healthcare policymakers totake some measures on this respect. Therefore, it’s endorsed that the higher consideration be given to disadvantaged areas and truthful distribution of healthcare assets. It can be important that the challenges and limitations to this entry be investigated in additional research as a result of, as said in different research, entry to well being providers for all folks is taken into account one of many main standards of wholesome societies, and there can be no sustainable growth within the case of continuance of the established order. Besides, the well being of communities is not going to proceed to enhance with out making a wholesome surroundings and with out provision of healthcare providers [52].
In our research, the ratio of lively beds to 10,000 folks in Kermanshah Province was 13.24. In a research carried out by Shahabi et al. [33], this index measured 15, 14.1 and 15.7 in Semnan, Yazd, ChaharmahalBakhtiari Provinces with essentially the most lively beds, versus Lorestan (5.40), Qom (5.40), Gilan (4.70) and Qazvin (6.10) with the fewest lively beds, respectively [33].
The ratio of lively beds to a inhabitants of 10,000 in every township is without doubt one of the vital indicators of well being. In this research, the outcomes demonstrated that the unequal distribution of lively beds at township ranges has been much like the outcomes of different research carried out in Iran [33, 53]. It is believed that the inappropriate distribution of well being assets in Kermanshah might have been because of the want for providers and the dearth of enough gear and human assets. Other research have proven that particular geographical circumstances and lack of welfare services may account for the dearth of hospitals with acceptable beds in townships [54]. In one other research, it was concluded that the insurance policies and plans resulting in the focus of actions and providers in giant cities accounted for this unequal distribution [55, 56].
The outcomes of the research demonstrated that the distribution of nurses to 10,000 folks throughout the townships in Kermanshah witnessed an inequality distribution. The outcomes of a research carried out in public hospitals of Iran indicated that the Semnan Province had the very best ratio of nurses to the inhabitants [21, 33], and Sistan and Baluchestan Provinces had the bottom ratio with 2.40 nurses, which was because of the location and space of every province, the dispersion of the inhabitants, and the variety of nurses [48].
In addition, the outcomes of the current research confirmed that the distribution of dentists to 10,000 folks within the Kermanshah Province measured 1.29. In a research carried out in Iran in 2010, the distribution of dentists was 2.90. Moreover, the outcomes indicated that the ratios of dentists to 10,000 folks measured seven in Tehran, 3.2 in Isfahan and three in Yazd, which have been the most important. However, this ratio measured 0.9 in Sistan and Baluchestan, 0.9 in Ardebil, and one in North and South Khorasan and Hormozgan, which have been the smallest [51].
Additionally, the outcomes of the current research demonstrated that the distribution of pharmacists to 10,000 folks within the Kermanshah Province measured 0.16. In a research carried out in Iran in 2010, this determine was 2.10. The highest variety of pharmacists in 10,000 folks was in Tehran (4.6), Isfahan (2.2) and East Azarbayejan (2.1), respectively. However, the bottom ratio of pharmacists to the inhabitants existed in Hormozgan (0.5) Sistan and Baluchestan (0.7), Kurdistan and South Khorasan (0.8), respectively [51].
In addition, the outcomes of the current research demonstrated that almost all nursing workers, paramedics, common practitioners and specialists belonged to Kermanshah per 10,000 folks, versus the fewest that belonged to the townships of Salas-e Babajani, Dalaho, and Ravansar. Shahabi et al. [33] additionally confirmed that there was an inequality within the distribution of those indexes amongst Iran’s provinces over 2001–2006 [33]. This was most likely because of the location and space of every township, the distribution of the inhabitants and the variety of medical personnel in township [55, 57]. Another attainable cause is perhaps the healthcare workers’s lack of willingness to serve in disadvantaged areas [58, 59]. It needs to be famous that, in response to Alla-Eddini et al. [58], within the case of offering physicians with sure circumstances equivalent to the quantity of revenue and sort of employment standing, they are going to be able to serve in disadvantaged areas.
The outcomes of cluster evaluation demonstrated that the townships of Kermanshah Province fall into three classes by way of the event in healthcare: Kermanshah, Qasar-e Shirin and Javanrood match into the developed class. While the undeveloped class included Ravansar, Dalaho and Salas-e BabajaniTownships (see Figure 1). The outcomes of research carried out in Kermanshah have been indicative of the truth that the townships of Qasr-eShirin, Kermanshah and Paveh have been privileged, whereas the townships of Sahneh, Dalaho and Salas-e Babajani have been disadvantaged. This discovering was not concurrent with the outcomes of research carried out by Rezai et al. [60]. Moreover, the outcomes of research, carried out at nation and provincial ranges, on the standing of entry to and correct distribution of well being assets have emphasised the existence of a vacuum and unequal and imbalanced distribution in healthcare providers and assets in Iran [55, 61, 62]. The growth indexes of healthcare providers haven’t been distributed equitably on a par with different growth indexes among the many geographical areas in creating nations [57, 63, 64]. Accordingly, there’s a hole within the growth of those indexes, which is clearly seen within the townships of Kermanshah Province. This scenario, as emphasised in different research, leads to regional inequalities in well being along with inequalities in entry to healthcare providers [55, 61, 62], that are primarily attributable to variations within the ranges of financial growth and variations in entry to numerous well being and medical services [17], thereby making residents of the deprived areas quickly migrate to giant cities for the good thing about services and providers, which require an excessive amount of time and bills [65]. Research has proven that selling healthcare methods and acceptable entry to medical care will result in eradicating poverty, educating girls, empowering girls, decreasing baby mortality charges, selling maternal well being, combating AIDS, Malaria and different ailments, thereby offering folks with sustainable well being [66]. Therefore, the well being policymakers ought to take into account the adjustment of this case in Kermanshah.
Given that GIS is helpful for assessing numerous spatial disparities [63] together with healthcare wants in addition to analyzing entry to well being providers and understanding inequalities amongst totally different places, and the truth that it’s a good software for evaluating well being insurance policies which result in reductions in well being prices and end in growth of well being on the neighborhood degree [70], it’s endorsed that this software be utilized in administration and promotion of well being within the Kermanshah Province.
Limitations
In this paper, the explanations for this lack of entry weren’t lined. Instead, the indexes have been addressed that defined the quantitative dimensions of well being growth, and provided that the qualitative dimensions of well being growth, which signify the standard of service supply, are additionally vital features of entry to medical care, it’s, subsequently, advised that the qualitative features of entry to well being providers needs to be addressed in future research, too. Furthermore, the size of inequality have been studied on the ranges of townships for the reason that inequality dimensions stay unknown largely at decrease ranges (rural and concrete) of nation divisions. Hence, it’s advised that the inequalities on the ranges of villages and cities be investigated in an effort to each clarify the variations between areas (townships) and make clear the inter-regional variations. We didn’t have entry to the statistics of the neighborhood well being staff on the native well being facilities positioned in rural. Also, the research reported on this paper has some limitations. For instance, socio-economic funds required, transport, willingness of well being providers to simply accept cultural minorities, bodily accessibility for folks with disabilities, gender issues, and cultural attitudes and beliefs about well being providers and their usefulness.
We have been unable to entry teams that require comparatively greater entry and use of well being providers than others—for instance, moms and infants and older folks or others within the inhabitants whose well being is comparatively extra at risk- for instance these with continual well being circumstances.
Conclusions
Easy entry to medical care is without doubt one of the important necessities in growth applications. Developing nations have allotted a smaller share of their assets to medical care because of numerous causes together with the dearth of nationwide well being planning, insufficient well being care system, and the insufficient issues within the well being sector. In this regard, we’re seeing a deep hole within the inequality of entry to medical care in creating nations. The province of Kermanshah was investigated as proof of this declare.
The indices of growth of services and healthcare assets within the Kermanshah province haven’t been distributed equitably and delicately balanced among the many townships and totally different geographical areas, and their distribution was not proportional to the inhabitants. Besides, regardless of enhancements in well being, many residents of the Kermanshah Province endure from inequality and poor entry to well being providers. Accordingly, it’s advised that the well being policymakers of the Kermanshah Province rethink the insurance policies on the equitable distribution of healthcare providers all through the province. It can be beneficial that precedence be given to underdeveloped townships towards provision of equal entry for the disadvantaged inhabitants to providers.
Data availability assertion
Ethics assertion
The research involving human individuals have been reviewed and permitted by Kermanshah University of Medical Sciences. The sufferers/individuals supplied their written knowledgeable consent to take part on this research. Written knowledgeable consent was obtained from the person(s) for the publication of any probably identifiable photos or knowledge included on this article.
Author contributions
Funding
This work was supported by the colleagues within the Kermanshah University of Medical Sciences, in addition to the monetary and religious helps of the Deputy Head of Research and Technology Department of the Kermanshah University of Medical Sciences are sincerely appreciated beneath Grant Number 92446.
Conflict of curiosity
Publisher’s observe
References
1. WHO. The World Health Report 2003: Shaping the Future. Geneva: World Health Organization (2003).
Google Scholar
2. Amini N, Yadolahi H. S. Ranking of nation provinces. Health Soc Welfare Q. (2006) 5:27–48.
Google Scholar
3. Van Minh H, Giang KB, Hoat LN, Chung LH, Huong TTG, Phuong NTK, et al. Analysis of chosen social determinants of well being and their relationships with maternal well being service protection and baby mortality in Vietnam. Glob Health Action. (2016) 9:1–9. doi: 10.3402/gha.v9.28836
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Gudes O, Kendall E, Yigitcanlar T, Pathak V, Baum S. Rethinking well being planning: a framework for organising data to underpin collaborative well being planning. Health Inform Manag J. (2010) 39:18–29. doi: 10.1177/183335831003900204
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Baum S, Kendall E, Muenchberger H, Gudes O, Yigitcanlar T. Geographical data methods: an efficient planning and decision-making platform for neighborhood well being coalitions in Australia. Health Inform Manag J. (2010) 39:28–33. doi: 10.1177/183335831003900305
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Teimouri R, Yigitcanlar T. An strategy in the direction of efficient ecological planning: quantitative evaluation of city inexperienced house traits. Glob J Environ Sci Manag. (2018) 4:195–206.
Google Scholar
8. Orueta JF, García-Álvarez A, Alonso-Morán E, Vallejo-Torres L, Nuño-Solinis R. Socioeconomic variation within the burden of continual circumstances and well being care provision-analyzing administrative particular person degree knowledge from the Basque Country, Spain. BMC Public Health. (2013) 13:870–6. doi: 10.1186/1471-2458-13-870
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Reshadat S, Zangeneh A, Saeidi S, Teimouri R, Yigitcanlar T. Measures of spatial accessibility to well being facilities: investigating city and rural disparities in Kermanshah, Iran. J Public Health. (2019) 27:519–29. doi: 10.1007/s10389-018-0966-9
CrossRef Full Text | Google Scholar
10. Reshadat S, Zangeneh A, Saeidi S, Ghasemi SR, Rajabi-Gilan N, Zakiei A. Inequalities in entry to hospitals: a case research within the Islamic Republic of Iran 1997–2012. Eastern Mediterranean Health J. (2018) 25:119–23. doi: 10.26719/emhj.18.061
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Reshadat S, Saedi S, Zangeneh A, Ghasemi S, Gilan N, Karbasi A, et al. Spatial accessibility of the inhabitants to city well being centres in Kermanshah, Islamic Republic of Iran: a geographic data methods evaluation. Eastern Mediterranean Health J. (2015) 21:389. doi: 10.26719/2015.21.6.389
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Carey G, Malbon E, Reeders D, Kavanagh A, Llewellyn G. Redressing or entrenching social and well being inequities via coverage implementation? Examining personalised budgets via the Australian National Disability Insurance Scheme. Int J Equity Health. (2017) 16:192. doi: 10.1186/s12939-017-0682-z
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Wisk LE, Sharma N. Inequalities in adolescent and younger grownup medical insurance protection and entry to well being care post-federal well being reform. J Adolt Health. (2018) 62:S19. doi: 10.1016/j.jadohealth.2017.11.038
CrossRef Full Text | Google Scholar
14. Janković J, Šiljak S, Erić M, Marinković J, Janković S. Inequalities within the utilization of well being care providers in a transition European nation: outcomes from the nationwide inhabitants well being survey. Int J Public Health. (2018) 63:261–72. doi: 10.1007/s00038-017-1009-y
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Culyer AJ, Newhouse JP. Handbook of Health Economics. New York: Elsevier (2000).
Google Scholar
16. Park JM. Equity within the utilization of doctor and inpatient hospital providers: proof from Korean well being panel survey. Int J Equity Health. (2016) 15:159–69. doi: 10.1186/s12939-016-0452-3
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Fang P, Dong S, Xiao J, Liu C, Feng X, Wang Y. Regional inequality in well being and its determinants: proof from China. Health Policy. (2010) 94:14–25. doi: 10.1016/j.healthpol.2009.08.002
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Rosen-Reynoso M, Porche MV, Kwan N, Bethell C, Thomas V, Robertson J, et al. Disparities in entry to easy-to-use providers for kids with particular well being care wants. Maternal Child Health J. (2016) 20:1041–53. doi: 10.1007/s10995-015-1890-z
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Liang D, Zhang D, Huang J, Schweitzer S. Does speedy and sustained financial progress result in convergence in well being assets the case of China From 1980 to 2010. J Health Care Organ Prov Financ. (2016) 53:1–20. doi: 10.1177/0046958016631699
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Ardelan A, Fatemi R, Alaedini F editors. The complete research of the efficient elements to estimate the required variety of common doctor in Iran. In: Proceed Health Economic Congress Evaluation, Iran (2002).
Google Scholar
23. Abolhasani F, Jamshidbeygi E, Mardfard N, Moghimi D, Maleki F. Report of Study the Rates of Represent the Health and Rehabilitation Services and Determination of Structural Characteristics and Geographical Distribution of Providing These Services Centers in 2002 and 2003. Tehran, Iran: Tandis Publication (2009).
Google Scholar
24. Mason T, Lau Y-S, Sutton M. Is the distribution of care high quality supplied beneath pay-for-performance equitable? Evidence from the Advancing Quality programme in England. Int J Equity Health. (2016) 15:156. doi: 10.1186/s12939-016-0434-5
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Iranian Council for Graduate Medical Education. The Report in Connection With Requires Specialist Number in Iran. Tehran: Ministry of Health and Medical Education (1999).
Google Scholar
26. WHO. The World Health Report 2008: Primary Health Care (Now More Than Ever). Geneva : World Health Organization (2014). p. 1–14. doi: 10.4102/phcfm.v1i1.112
CrossRef Full Text | Google Scholar
28. Inoue Ok, Matsumoto M, Toyokawa S, Kobayashi Y. Transition of doctor distribution (1980-2002) in Japan and elements predicting future rural apply. Rural Remote Health. (2009) 9:1070–5. doi: 10.22605/RRH1070
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Moscovice I. Policy Approaches for enhancing the distribution of physicians. Health Serv Res. (1983) 18:270.
Google Scholar
31. Carter R. The relation between private traits of physicians and apply location in Manitoba. CMAJ Canadian Med Associat J. (1987) 136:366–8.
PubMed Abstract | Google Scholar
32. Farzadfar F, Naghavi M, Sepanlou SG, Moghaddam SS, Dangel WJ, Weaver ND, et al. Health system efficiency in Iran: a scientific evaluation for the Global Burden of Disease Study 2019. Lancet. (2022) 399:1625–45. doi: 10.1016/S0140-6736(21)02751-3
PubMed Abstract | CrossRef Full Text | Google Scholar
33. Shahabi M, Tofighi S, Maleki M. The nurse and specialist physicians manpower distribution by inhabitants and its relationship with the variety of beds at public hospitals in Iran’s 2001–2006. J Health Administr. (2010) 13:7–14.
Google Scholar
34. Mehrjardi MHT, Mybodi HB, Sharifabadi AM. Investigation and rating of Iranian provinces by way of entry to well being sector indicators. Director General. (2012) 9:356–65.
Google Scholar
35. Khademi N, Reshadat S, Zangeneh A, Saeidi S, Ghasemi S, Rajabi-Gilan N, et al. A comparative research of the spatial distribution of HIV prevalence within the metropolis of < metropolis>Kermanshah < /metropolis>, Iran, in 1996–2014 utilizing geographical data methods. HIV Med. (2016) 18:137–42. doi: 10.1111/hiv.12416
PubMed Abstract | CrossRef Full Text | Google Scholar
36. Reshadat S, Saeidi S, Zangeneh AR, Khademi N, Khasi Ok, Ghasemi S, et al. Spatiotemporal Distribution of Gastrointestinal Tract Cancer via GIS over 2007–2012 in Kermanshah-Iran. Asian Pacific J Cancer Prev. (2015) 16:7737–42. doi: 10.7314/APJCP.2015.16.17.7737
PubMed Abstract | CrossRef Full Text | Google Scholar
38. Yadollahi M, Ghiassee A, Anvar M, Ghaem H, Farahmand M. Analysis of Shahid Rajaee hospital administrative knowledge on accidents ensuing from automotive accidents in Shiraz, Iran: 2011–2014 knowledge. Chinese J Traumatol. (2017) 20:27–33. doi: 10.1016/j.cjtee.2015.10.006
PubMed Abstract | CrossRef Full Text | Google Scholar
39. Reshadat S, Zangeneh A, Saeidi S, Ghasemi SR, Rajabi Gilan N, Abbasi S. Investigating the financial, social and cultural elements influencing complete fertility charge in Kermanshah. J Mazandaran Univ Med Sci. (2015) 25:108–12.
Google Scholar
41. Teoh WL, Khoo MB, Castagliola P, Yeong WC, Teh S. Run-sum management charts for monitoring the coefficient of variation. European J Operat Res. (2017) 257:144–58. doi: 10.1016/j.ejor.2016.08.067
CrossRef Full Text | Google Scholar
42. Köhn HF, Hubert LJ. Hierarchical cluster evaluation. Wiley StatsRef: Statistics Reference Online. (2006).
Google Scholar
43. McGillivray M. The human growth index: one more redundant composite growth indicator? World Develop. (1991) 19:1461–8. doi: 10.1016/0305-750X(91)90088-Y
CrossRef Full Text | Google Scholar
44. Shojaei P, Ghanbarzadegan A, Najibi M, Bastani P. Ranking of Iranian provinces primarily based on healthcare infrastructures: earlier than and after implementation of Health Transformation Plan. Cost Eff Resour Alloc. (2020) 18:1–3. doi: 10.1186/s12962-020-0204-5
PubMed Abstract | CrossRef Full Text | Google Scholar
45. Nobakht S, Shirdel A, Molavi-Taleghani Y, Doustmohammadi MM, Sheikhbardsiri H. Human assets for well being: A story overview of adequacy and distribution of medical and nonclinical human assets in hospitals of Iran. Int J of Health Plann and Manage. (2018) 33:560–72. doi: 10.1002/hpm.2510
PubMed Abstract | CrossRef Full Text | Google Scholar
46. Ziari Ok, Saeedi Rezvani N, Salehpour L. Measuring the diploma of growth of the Eastern Azerbaijan province metropolis (HDI). Product Manag. (2010) 3:75–95.
Google Scholar
47. Reshadat S, Zangeneh A, Saeidi S, Khademi N, Izadi N, Ghasemi SR, et al. The spatial clustering evaluation of HIV and poverty via gis within the metropolis of Kermansha, Western Iran. Acta Med Mediterranea. (2016) 32:1995–9.
Google Scholar
48. World Health Statistics. Global Health Indicators. Geneva: World Health Organization (2015). p. 40–160.
Google Scholar
49. Karimi I, Salarian A, Anbari Z. A comparative research on fairness in entry to well being providers in developed nations and designing a mannequin for Iran. Arak Medical Univ J. (2010) 12:92–104.
Google Scholar
50. Nasiripour AA, Maleki MR, Tabibi SJ, Chimeh EE. Factors affect on geographic distribution of physicians in chosen nations: a overview article. J Kermanshah Univ Med Sci. (2013) 17:600–10.
Google Scholar
51. Haghdoost AA, Kamyabi A, Sgrabad Ahad A, Sadeghirad B, Shafieyan H. Geographical distribution of various teams of the medical neighborhood within the nation and regional inequalities. J Med Council Islamic Republic Iran. (2010) 28:411–9.
Google Scholar
53. Sayyari A. Health Vision in Iran and Word. Science Future J. (2004) 1:50–9.
Google Scholar
54. Mostafavi H, Aghlmand S, Zandiyan H, Alipoori Sakha M, Bayati M, Mostafavi S. Inequitable distribution of specialists and hospital beds in West Azerbaijan Province. J Payavard Salamat. (2015) 9:55–66.
Google Scholar
55. Taghvaei M, Shahivandi A. Spatial distribution of well being providers in Iranian cities. Soc Welfare. (2011) 10:33–54.
PubMed Abstract | Google Scholar
56. Mohammadi M, Ziapoor A, Mahboubi M, Faroukhi A, Amani N, Hydarpour F, et al. Performance analysis of hospitals beneath supervision of Kermanshah medical sciences utilizing pabonlasoty diagram of a five-year interval (2008–2012). Life Sci J. (2014) 11:77–81.
Google Scholar
57. Zarabi A, Mohammadi J. Spatial evaluation of growth indicators of well being care. J Soci Welfare. (2008) 7:213–34.
Google Scholar
58. Alla-Eddini F, Fatemi R, Ranjbaran Jahromi H, Asghari E, Eskandari S, Ardalan A, et al. Iranian physicians’ willingness to work in underserved areas and associated elements in 2001. Razi J Med Sci. (2004) 11:247–55.
Google Scholar
59. Rabinowitz HK, Diamond JJ, Markham FW, Hazelwood CE. A program to extend the variety of household physicians in rural and underserved areas: impression after 22 years. JAMA. (1999) 281:255–60. doi: 10.1001/jama.281.3.255
PubMed Abstract | CrossRef Full Text | Google Scholar
60. Rezaei S, Ghazanfari S, Kazemi Z, Karyani AK. Access to healthcare services: case research of Kermanshah province. J Kermanshah Univ Med Sci. (2014) 18:416–25.
Google Scholar
61. Sulaimany A, Masum MG, Riahi V. The growth degree of well being indicators in Kermanshah province from the angle of social justice in 2010. J Kermanshah Univ Med Sci. (2014) 17:647–56.
Google Scholar
62. Bahadori M, Shams L, Sadeghifar J, Hamouzadeh P, Nejati M. Classification of well being structural indicators utilizing scalogram mannequin in Golestan province, Northern Iran. Iran J Public Health. (2012) 41:58–65.
PubMed Abstract | Google Scholar
63. Dummer TJ, Cook IG. Health in China and India: a cross-country comparability in a context of speedy globalisation. Soc Sci Med. (2008) 67:590–605. doi: 10.1016/j.socscimed.2008.04.019
PubMed Abstract | CrossRef Full Text | Google Scholar
64. Gauri V. Social rights and economics: claims to well being care and training in creating nations. World Develop. (2004) 32:465–77. doi: 10.1016/j.worlddev.2003.07.009
CrossRef Full Text | Google Scholar
65. Zarrabi A, Shaykh Baygloo R. Classification of Provinces of Iran by well being indicators. Soc Welfare. (2011) 11:107–28.
Google Scholar
66. Baldacci E, Clements B, Gupta S, Cui Q. Social spending, human capital, and progress in creating nations. World Develop. (2008) 36:1317–41. doi: 10.1016/j.worlddev.2007.08.003
CrossRef Full Text | Google Scholar
67. Kazemi A, Rezapoor A, Faradonbeh S, Nakhaei M, Ghazanfari S. Study the event degree of provinces in Iran: a concentrate on well being indicators. J Health Administrat. (2015) 18:59.
Google Scholar
68. Rostaei S, Ahadnejad Reveshty M, Asghari Zamani A, Zangenh A. Assessment of Urban Poverty Spatial Distribution in Kermanshah City. Soc Welfare. (2012) 12:77–101.
Google Scholar
69. Izadi N, Khoramdad M, Jamshidi P, Shafiei J, Firouzi A. Epidemiological sample and mortality charge development of street visitors accidents in Kermanshah Province (2009–2014). J Community Health Res. (2016) 5:158–68. doi: 10.5812/traumamon.39880
CrossRef Full Text | Google Scholar